
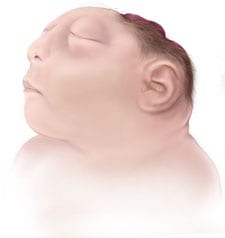
Anencephaly is the absence of a major portion of the brain, skull, and scalp that occurs during embryonic development. It is a cephalic disorder that results from a neural tube defect that occurs when the rostral (head) end of the neural tube fails to close, usually between the 23rd and 26th day following conception. Strictly speaking, the Greek term translates as "no in-head" (that is, totally lacking the inside part of the head, i.e., the brain), but it is accepted that children born with this disorder are in fact usually only lacking a telencephalon, the largest part of the brain consisting mainly of the cerebral hemispheres, including the neocortex, which is responsible for cognition. The remaining structure is usually covered only by a thin layer of membraneâ€" skin, bone, meninges, etc. are all lacking. With very few exceptions, infants with this disorder do not survive longer than a few hours or possibly days after their birth.
Signs and symptoms

The National Institute of Neurological Disorders and Stroke (NINDS) describes the presentation of this condition as follows: "A baby born with anencephaly is usually blind, deaf, unaware of its surroundings and unable to feel pain. Although some individuals with anencephaly may be born with a main brain stem, the lack of a functioning cerebrum permanently rules out the possibility of ever gaining awareness of their surroundings. Reflex actions such as breathing and responses to sound or touch may occur."
Causes
The cause of anencephaly is disputed.
Folic acid has been shown to be important in neural tube formation since at least 1995, and as a subtype of neural tube defect, folic acid may play a role in anencephaly. Studies have shown that the addition of folic acid to the diet of women of child-bearing age may significantly reduce, although not eliminate, the incidence of neural tube defects. Therefore, it is recommended that all women of child-bearing age consume 0.4Â mg of folic acid daily, especially those attempting to conceive or who may possibly conceive, as this can reduce the risk to 0.03%. It is not advisable to wait until pregnancy has begun, since, by the time a woman knows she is pregnant, the critical time for the formation of a neural tube defect has usually already passed. A physician may prescribe even higher dosages of folic acid (4Â mg/day) for women having had a previous pregnancy with a neural tube defect.
In general, neural tube defects do not follow direct patterns of heredity, though there is some indirect evidence of inheritance, and recent animal models indicate a possible association with deficiencies of the transcription factor TEAD2. Studies show that a woman who has had one child with a neural tube defect such as anencephaly has about a 3% risk of having another child with a neural tube defect, as opposed to the background rate of 0.1% occurrence in the population at large.Genetic counseling is usually offered to women at a higher risk of having a child with a neural tube defect to discuss available testing.
It is known that women taking certain medications for epilepsy and women with insulin-dependent diabetes have a higher risk of having a child with a neural tube defect.
Anencephaly and other physical and mental deformities have also been blamed on a high exposure to such toxins as lead, chromium, mercury, and nickel.
Relation to genetic ciliopathy
Until recently, medical literature did not indicate a connection among many genetic disorders, both genetic syndromes and genetic diseases, that are now being found to be related. As a result of new genetic research, some of these are, in fact, highly related in their root cause despite the widely varying set of medical symptoms that are clinically visible in the disorders. Anencephaly is one such disease, part of an emerging class of diseases called ciliopathies. The underlying cause may be a dysfunctional molecular mechanism in the primary cilia structures of the cell, organelles present in many cellular types throughout the human body. The cilia defects adversely affect "numerous critical developmental signaling pathways" essential to cellular development and, thus, offer a plausible hypothesis for the often multi-symptom nature of a large set of syndromes and diseases. Known ciliopathies include primary ciliary dyskinesia, Bardet-Biedl syndrome, polycystic kidney and liver disease, nephronophthisis, Alström syndrome, Meckel-Gruber syndrome, and some forms of retinal degeneration.
Diagnosis
Anencephaly can often be diagnosed before birth through an ultrasound examination. The maternal serum alpha-fetoprotein (AFP screening) and detailed fetal ultrasound can be useful for screening for neural tube defects such as spina bifida or anencephaly.
Meroanencephaly
Meronanencephaly is a rare form of anencephaly characterized by malformed cranial bones, a median cranial defect, and a cranial protrusion called area cerebrovasculosa. Area cerebrovasculosa is a section of abnormal, spongy, vascular tissue admixed with glial tissue ranging from simply a membrane to a large mass of connective tissue, hemorrhagic vascular channels, glial nodules, and disorganized choroid plexuses.
Holo anencephaly
The most common type of anencephaly, in which the brain is completely absent.
Craniorachischisis
The most severe type of anencephaly where area cerebrovasculosa and area medullovasculosa fill both cranial defects and the spinal column. Craniorachischisis is characterized by anencephaly accompanied by bony defects in the spine and the exposure of neural tissue as the vault of the skull fails to form. Craniorachischisis occurs in about 1 of every 1000 live births, but various physical and chemical tests can detect neural tube closure during early pregnancy.
Prognosis

There is no cure or standard treatment for anencephaly and the prognosis for patients is death. Most anencephalic fetuses do not survive birth, accounting for 55% of non-aborted cases. If the infant is not stillborn, then he or she will usually die within a few hours or days after birth from cardiorespiratory arrest.
Three recorded cases of anencephalic children surviving for longer periods of time are Stephanie Keene of Falls Church, Virginia, who lived for 2 years 174 days; Vitoria de Cristo, born in Brazil in January 2010 and surviving until July 17, 2012; Nickolas Coke of Pueblo, Colorado, who lived for 3 years and 11 months, died October 31, 2012;
In almost all cases, anencephalic infants are not aggressively resuscitated because there is no chance of the infant's ever achieving a conscious existence. Instead, the usual clinical practice is to offer hydration, nutrition, and comfort measures and to "let nature take its course". Artificial ventilation, surgery (to fix any co-existing congenital defects), and drug therapy (such as antibiotics) are usually regarded as futile efforts. Some clinicians and medical ethicists view even the provision of nutrition and hydration as medically futile.
Epidemiology
In the United States, anencephaly occurs in about 1 out of every 10,000 births. Research has suggested that, overall, female babies are more likely to be affected by the disorder.
Ethical issues
Organ donation
One issue concerning anencephalic newborns is organ donation. Initial legal guidance came from the case of Baby Theresa in 1992, in which the boundaries of organ donation were tested for the first time. Infant organs are scarce, and the high demand for pediatric organ transplants poses a major public health issue. In 1999, it was found that among children who die under the age of two, thirty to fifty percent do so while awaiting transplant. In order for infant organs to be viable and used for transplant, they must be removed while the infant still has circulation or very soon after circulation has ceased. However, this poses both legal and ethical issues. In the United States, all states have laws that forbid the removal of organs from a donor until after the donor has died, except in the case of altruistic living donations of a kidney or liver segment.
The goal of those in support of organ donation is that it will further contribute to the pool of suitable organs for transplants while the need for lifesaving organ transplants is so great. It has been estimated that 400â€"500 infant hearts and kidneys and 500-1,000 infant livers are needed in the United States each year. Because anencephalic neonates have partially functioning brain stems, they possess some brain stem reflexes such as spontaneous respirations. For this reason, these patients cannot be declared brain dead.
Within the medical community, the main ethical issues with organ donation are a misdiagnosis of anencephaly, the slippery slope argument, that anencephalic neonates would rarely be a source of organs, and that it would undermine confidence in organ transplantation. Slippery slope concerns are a major issue in personhood debates, across the board. In regards to anencephaly, those who oppose organ donation argue that it could open the door for involuntary organ donors such as an elderly person with severe dementia. Another point of contention is the number of children who would actually benefit. There are discrepancies in statistics; however, it is known that most anencephalic children are stillborn.
Proposals have been made to bypass the legal and ethical issues surrounding organ donation. These include waiting for death to occur before procuring organs, expanding the definition of death, creating a special legal category for anencephalic infants, and defining them as non-persons.
Brain death
There are four different concepts used to determine brain death: failure of heart, failure of lungs, whole brain death, and neocortical death. Some argue that anencephalics experience neocortical death, in which there is an irreversible loss of consciousness and self-awareness, two determinants of a person. Brain death is another source of support for organ donation.
Neocortical death, similar to a persistent vegetative state (PVS), involves loss of cognitive functioning of the brain. A proposal by law professor David Randolph Smith, in an attempt to prove that neocortical death should legally be treated the same as brain death, involved PET scans to determine the similarities. However this proposal has been criticized on the basis that confirming neocortical death by PET scan may risk indeterminacy.
Pregnancy termination
Anencephaly can be diagnosed prenatally with a high degree of accuracy. Given that anencephaly is a fatal condition, parents receive the option of abortion in either the second or the third trimester of pregnancy, depending on the abortion laws in the state. In 2012, Brazil extended the right of abortion to mothers with anencephalic fetuses. This decision is, however, receiving much disapproval by several religious groups.
Legal proceedings
The case of baby Theresa was the beginning of the ethical debate over anencephalic infant organ donation. The story of baby Theresa remains a focus of basic moral philosophy. Baby Theresa was born with anencephaly in 1992. Her parents, knowing that their child was going to die, requested that her organs be given for transplantation. Although her physicians agreed, Florida law prohibited the infant's organs from being removed while she was still alive. By the time she died nine days after birth, her organs had deteriorated past the point of being viable.
Baby K was an anenecephalic infant that was kept alive for two years and 174 days under intensive care by order of the US Court of Appeals for the Fourth Circuit.
United States Uniform Acts
The Uniform Determination of Death Act (UDDA) is a model bill, adopted by many US states, stating that an individual who has sustained either 1) irreversible cessation of circulatory and respiratory functions or 2) irreversible cessation of all functions of the entire brain, including the brain stem, is dead. This bill was a result of much debate over the definition of death and is applicable to the debate over anencephaly. A related bill, the Uniform Anatomical Gift Act (UAGA), grants individuals and, after death, their family members the right to decide whether or not to donate organs. Because it is against the law for any person to pay money for an organ, the person in need of an organ transplant must rely on a volunteer.
There have been two state bills that proposed to change current laws regarding death and organ donation. California Senate Bill 2019 proposed to amend the UDDA to define anencephalic infants as already dead, while New Jersey Assembly Bill 3367 proposed to allow anencephalic infants to be organ sources even if they are not dead.
Research
Some genetic research has been conducted to determine the causes of anencephaly. It has been found that cartilage homeoprotein (CART1) is selectively expressed in chondrocytes (cartilage cells). The CART1 gene to chromosome 12q21.3â€"q22 has been mapped. Also, it has been found that mice homozygous for deficiency in the Cart1 gene manifested acrania and meroanencephaly, and prenatal treatment with folic acid will suppress acrania and meroanencephaly in the Cart1-deficient mutants.
References
External links

- Genetic Basis of Anencephaly
- Anencephaly Net. Encourages women to carry anencephalic babies to term and let them die post birth or in utero.
- Exencephaly â€" Anencephaly Sequence and its Sonographic Features
- Anencephaly info. General information. Encourages women to carry anencephalic infants to term and "...share the stories of the brief, but wonderful lives of babies with anencephaly." Includes
- Anencephalie-info.org. General information on anencephalic babies carried to term, including life expectancy.
- Duke University's Anencephaly page, including recruiting information for research
- Images of Anencephaly
- Specimens â€" Anencephaly






0 comments:
Post a Comment