Chromoblastomycosis (also known as chromomycosis, cladosporiosis, Fonseca's disease, Pedroso's disease, phaeosporotrichosis, or verrucous dermatitis) is a long-term fungal infection of the skin and subcutaneous tissue (a chronic subcutaneous mycosis). The infection occurs most commonly in tropical or subtropical climates, often in rural areas. It can be caused by many different types of fungi which become implanted under the skin, often by thorns or splinters. Chromoblastomycosis spreads very slowly; it is rarely fatal and usually has a good prognosis, but it can be very difficult to cure. The several treatment options include medication and surgery.
Features
The initial trauma causing the infection is often not noticed or forgotten. The infection builds at the site over a period of years, and a small red papule (skin elevation) appears. The lesion is usually not painful, with few, if any symptoms. Patients rarely seek medical care at this point.
Several complications may occur. Usually, the infection slowly spreads to the surrounding tissue while still remaining localized to the area around the original wound. However, sometimes the fungi may spread through the blood vessels or lymph vessels, producing metastatic lesions at distant sites. Another possibility is secondary infection with bacteria. This may lead to lymph stasis (obstruction of the lymph vessels) and elephantiasis. The nodules may become ulcerated, or multiple nodules may grow and coalesce, affecting a large area of a limb.
Pathophysiology

Chromoblastomycosis is believed to originate in minor trauma to the skin, usually from vegetative material such as thorns or splinters; this trauma implants fungi in the subcutaneous tissue. In many cases, the patient will not notice or remember the initial trauma, as symptoms often do not appear for years. The fungi most commonly observed to cause chromoblastomycosis are:
- Fonsecaea pedrosoi
- Phialophora verrucosa
- Cladosporium carrionii
- Fonsecaea compacta
Over months to years, an erythematous papule appears at the site of inoculation. Although the mycosis slowly spreads, it usually remains localized to the skin and subcutaneous tissue. Hematogenous and/or lymphatic spread may occur. Multiple nodules may appear on the same limb, sometimes coalescing into a large plaque. Secondary bacterial infection may occur, sometimes inducing lymphatic obstruction. The central portion of the lesion may heal, producing a scar, or it may ulcerate.
Diagnosis

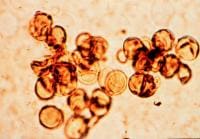
The most informative test is to scrape the lesion and add potassium hydroxide (KOH), then examine under a microscope. (KOH scrapings are commonly used to examine fungal infections.) The pathognomonic finding is observing medlar bodies, sclerotic cells. Scrapings from the lesion can also be cultured to identify the organism involved. Blood tests and imaging studies are not commonly used.
On histology, chromoblastomycosis manifests as pigmented yeasts resembling "copper pennies". Special stains, such as periodic acid schiff and Gömöri methenamine silver, can be used to demonstrate the fungal organisms if needed.
Treatment

Chromoblastomycosis is very difficult to cure. The primary treatments of choice are:
- Itraconazole, an antifungal azole, is given orally, with or without flucytosine.
- Alternatively, cryosurgery with liquid nitrogen has also been shown to be effective.
Other treatment options are the antifungal drug terbinafine, an experimental drug posaconazole, and heat therapy.
Antibiotics may be used to treat bacterial superinfections.
Amphotericin B has also been used.
Prognosis

The prognosis for chromoblastomycosis is very good for small lesions. Severe cases are difficult to cure, although the prognosis is still quite good. The primary complications are ulceration, lymphedema, and secondary bacterial infection. A few cases of malignant transformation to squamous cell carcinoma have been reported. Chromoblastomycosis is very rarely fatal.
Prevention

No preventive measure is known aside from avoiding the traumatic inoculation of fungi. At least one study found a correlation between walking barefoot in endemic areas and occurrence of chromoblastomycosis on the foot.
Epidemiology
Chromoblastomycosis occurs around the world, but is most common in rural areas between approximately 30°N and 30°S latitude. Madagascar and Japan have the highest incidence. Over two-thirds of patients are male, and usually between the ages of 30 and 50. A correlation with HLA-A29 suggests genetic factors may play a role, as well.





0 comments:
Post a Comment