
Cryptosporidiosis, also known as crypto, is a parasitic disease caused by Cryptosporidium, a protozoan parasite in the phylum Apicomplexa. It affects the intestines and is typically an acute short-term infection. It is spread through the fecal-oral route, often through contaminated water; the main symptom is self-limiting diarrhea in people with intact immune systems. In immunocompromised individuals, such as AIDS patients, the symptoms are particularly severe and often fatal.
Cryptosporidium is the organism most commonly isolated in HIV-positive patients presenting with diarrhea. Treatment is symptomatic, with fluid rehydration, electrolyte correction and management of any pain. Despite not being identified until 1976, it is one of the most common waterborne diseases and is found worldwide. The parasite is transmitted by environmentally hardy microbial cysts (oocysts) that, once ingested, exist in the small intestine and result in an infection of intestinal epithelial tissue.
Signs and symptoms

Symptoms appear from two to ten days after infection, with an average of 7 days, and last for up to two weeks, or in some cases, up to one month. There are 3 possible forms of the illness in immunocompetent people. The disease can be tragic or cause acute diarrhea or persistent diarrhea that can last for a few weeks. Diarrhea is usually watery with mucus. It is very rare to find blood or leukocytes in the diarrhea.
As well as watery diarrhea, there is often stomach pains or cramps and a low fever. Other symptoms include nausea, vomiting, malabsorption and dehydration. Asymptomatic individuals (those with no symptoms) are nevertheless infective, and thus can pass on the infection to others. Even after symptoms have finally subsided, an individual is still infective for some weeks.
Severe diseases, including pancreatitis, can occur.
Immunocompromised people, as well as very young or very old people, can develop a more severe form of cryptosporidiosis. There are 4 clinical presentations for patients with AIDS. 4% have no symptoms, 29% have a transient infection, 60% have chronic diarrhea, and 8% have a severe, cholera-like infection. With transient infections diarrhea ends within 2 months and Cryptosporidium is no longer found in the feces. Chronic diarrhea is diarrhea that lasts for 2 or more months. The most severe form results in the patients excreting at least 2 liters of watery diarrhea per day. They can lose up to 25 liters per day. AIDS patients can have up to 10 stools per day. They experience severe malabsorption and can have 10% weight loss. Many of them never completely eliminate Cryptosporidium from their bodies.
When Cryptosporidium spreads beyond the intestine, as it can predominantly in patients with AIDS, it can reach the lungs, middle ear, pancreas, and stomach. Thus, one symptom is pain in the right upper quadrant. The parasite can infect the biliary tract, causing biliary cryptosporidiosis. This can result in cholecystitis and cholangitis.
Cause
Cryptosporidium is a protozoan pathogen of the Phylum Apicomplexa and causes a diarrheal illness called cryptosporidiosis. Other apicomplexan pathogens include the malaria parasite Plasmodium, and Toxoplasma, the causative agent of toxoplasmosis. Unlike Plasmodium, which transmits via a mosquito vector, Cryptosporidium does not require an insect vector and is capable of completing its life cycle within a single host, resulting in microbial cyst stages that are excreted in feces and are capable of transmission to a new host. However, studies show that synanthropic filth flies may be involved in the transmission of human and animal cryptosporidiosis.
The pattern of Cryptosporidium life cycle fits well that of other intestinal homogeneous coccidian genera of the suborder Eimeriina: macro- and microgamonts develop independently; a microgamont gives rise to numerous male gametes; and oocysts serving for parasites' spreading in the environment.
Electron microscopic studies made from the 1970s have shown the intracellular, although extracytoplasmic localization of Cryptosporidium species.
These species possess a number of unusual features:
- an endogenous phase of development in microvilli of epithelial surfaces
- two morphofunctional types of oocysts
- the smallest number of sporozoites per oocyst
- a multi-membraneous "feeder" organelle
DNA studies suggest a relationship with the gregarines rather than the coccidia. The taxonomic position of this group has not yet been finally agreed upon.
The genome of Cryptosporidium parvum was sequenced in 2004 and was found to be unusual amongst Eukaryotes in that the mitochondria seem not to contain DNA. A closely related species, C. hominis, also has its genome sequence available. CryptoDB.org is a NIH-funded database that provides access to the Cryptosporidium genomics data sets.
A number of Cryptosporidium infect mammals. In humans, the main causes of disease are C. parvum and C. hominis (previously C. parvum genotype 1). C. canis, C. felis, C. meleagridis, and C. muris can also cause disease in humans.
Cryptosporidiosis is typically an acute short-term infection but can become severe and non-resolving in children and immunocompromised individuals. In humans, it remains in the lower intestine and may remain for up to five weeks. The parasite is transmitted by environmentally hardy microbial cysts (oocysts) that, once ingested, exist in the small intestine and result in an infection of intestinal epithelial tissue.
Transmission
Infection is through contaminated material such as earth, water, uncooked or cross-contaminated food that has been in contact with the feces of an infected individual or animal. Contact must then be transferred to the mouth and swallowed. It is especially prevalent amongst those in regular contact with bodies of fresh water including recreational water such as swimming pools. Other potential sources include insufficiently treated water supplies, contaminated food, or exposure to feces. The high resistance of Cryptosporidium oocysts to disinfectants such as chlorine bleach enables them to survive for long periods and still remain infective. Some outbreaks have happened in day care related to diaper changes.
The following groups have an elevated risk of being exposed to Cryptosporidium:
- People who swim regularly in pools with insufficient sanitation (certain strains of Cryptosporidium are chlorine-resistant)
- Child care workers
- Parents of infected children
- People who take care of other people with cryptosporidiosis
- International travelers
- Backpackers, hikers, and campers who drink unfiltered, untreated water
- People, including swimmers, who swallow water from contaminated sources
- People who handle infected cattle
- People exposed to human feces through sexual contact
Cases of cryptosporidiosis can occur in a city that does not have a contaminated water supply. In a city with clean water, it may be that cases of cryptosporidiosis have different origins. Testing of water, as well as epidemiological study, are necessary to determine the sources of specific infections. Note that Cryptosporidium typically does not cause serious illness in healthy people. It may chronically sicken some children, as well as adults who are exposed and immunocompromised. A subset of the immunocompromised population is people with AIDS. Some sexual behaviours can transmit the parasite directly.
Life cycle
Cryptosporidium has a spore phase (oocyst) and in this state it can survive for lengthy periods outside a host. It can also resist many common disinfectants, notably chlorine-based disinfectants.
The life cycle of Cryptosporidium parvum consists of an asexual stage and a sexual stage. After being ingested, the oocysts excyst in the small intestine. They release sporozoites that attach to the microvilli of the epithelial cells of the small intestine. From there they become trophozoites that reproduce asexually by multiple fission, a process known as schizogony. The trophozoites develop into Type 1 meronts [1] that contain 8 daughter cells.
These daughter cells are Type 1 merozoites, which get released by the meronts. Some of these merozoites can cause autoinfection by attaching to epithelial cells. Others of these merozoites become Type II meronts, which contain 4 Type II merozoites. These merozoites get released and they attach to the epithelial cells. From there they become either macrogamonts or microgamonts. These are the female and male sexual forms, respectively. This stage, when sexual forms arise, is called gametogony.
Zygotes are formed by microgametes from the microgamont penetrating the macrogamonts. The zygotes develop into oocysts of two types. 20% of oocysts have thin walls and so can reinfect the host by rupturing and releasing sporozoites that start the process over again. The thick-walled oocysts are excreted into the environment. The oocysts are mature and infective upon being excreted. They can survive in the environment for months.
Pathogenesis

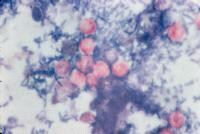
The oocysts are ovoid or spherical and measure 5 to 6 micrometers across. When in flotation preparations they appear highly refractile. The oocysts contains up to 4 sporozoites that are bow-shaped.
As few as 2 to 10 oocysts can initiate an infection. The parasite is located in the brush border of the epithelial cells of the small intestine. They are mainly located in the jejunum. When the sporozoites attach the epithelial cells’ membrane envelops them. Thus, they are “intracellular but extracytoplasmicâ€. The parasite can cause damage to the microvilli where it attaches. The infected human excretes the most oocysts during the first week. Oocysts can be excreted for weeks after the diarrhea subsides.
The immune system reduces the formation of Type 1 merozoites as well as the number of thin-walled oocysts. This helps prevent autoinfection. B cells do not help with the initial response or the fight to eliminate the parasite.
Diagnosis
There are many diagnostic tests for Cryptosporidium. They include microscopy, staining, and detection of antibodies. Microscopy can help identify oocysts in fecal matter. To increase the chance of finding the oocysts, the diagnostician should inspect at least 3 stool samples. There are several techniques to concentrate either the stool sample or the oocysts. The modified formalin-ethyl acetate (FEA) concentration method concentrates the stool. Both the modified zinc sulfate centrifugal flotation technique and the Sheather’s sugar flotation procedure can concentrate the oocysts by causing them to float. Another form of microscopy is fluorescent microscopy done by staining with auramine.
Other staining techniques include acid-fast staining, which will stain the oocysts red. One type of acid-fast stain is the Kinyoun technique. Giemsa staining can also be performed. Part of the small intestine can be stained with hematoxylin and eosin (H & E), which will show oocysts attached to the epithelial cells.
Detecting antigens is yet another way to diagnose the disease. This can be done with direct fluorescent antibody (DFA) techniques. It can also be achieved through indirect immunofluorescence assay. Enzyme-Linked ImmunoSorbent Assay (ELISA) also detects antigens.
Polymerase chain reaction (PCR) is another way to diagnose cryptosporidiosis. It can even identify the specific species of Cryptosporidium. If the patient is thought to have biliary cryptosporidiosis, then an appropriate diagnostic technique is ultrasonography. If that returns normal results, the next step would be to perform endoscopic retrograde cholangiopancreatography.
Prevention
Many treatment plants that take raw water from rivers, lakes, and reservoirs for public drinking water production use conventional filtration technologies. This involves a series of processes, including coagulation, flocculation, sedimentation, and filtration. Direct filtration, which is typically used to treat water with low particulate levels, includes coagulation and filtration, but not sedimentation. Other common filtration processes, including slow sand filters, diatomaceous earth filters and membranes will remove 99% of Cryptosporidium. Membranes and bag and cartridge filters remove Cryptosporidium product-specifically.
While Cryptosporidium is highly resistant to chlorine disinfection, with high enough concentrations and contact time, Cryptosporidium will be inactivated by chlorine dioxide and ozone treatment. The required levels of chlorine generally preclude the use of chlorine disinfection as a reliable method to control Cryptosporidium in drinking water. Ultraviolet light treatment at relatively low doses will inactivate Cryptosporidium. Water Research Foundation-funded research originally discovered UV's efficacy in inactivating Cryptosporidium.
One of the largest challenges in identifying outbreaks is the ability to identify Cryptosporidium in the laboratory. Real-time monitoring technology is now able to detect Cryptosporidium with online systems, unlike the spot and batch testing methods used in the past.
The most reliable way to decontaminate drinking water that may be contaminated by Cryptosporidium is to boil it.
In the US the law requires doctors and labs to report cases of cryptosporidiosis to local or state health departments. These departments then report to the Center for Disease Control and Prevention. The best way to prevent getting and spreading cryptosporidiosis is to have good hygiene and sanitation. An example would be hand-washing. Prevention is through washing hands carefully after going to the bathroom or contacting stool, and before eating. People should avoid contact with animal feces. They should also avoid possibly contaminated food and water. In addition, people should refrain from engaging in sexual activities that can expose them to feces.
Standard water filtration may not be enough to eliminate Cryptosporidium; boiling for at least 1 minute (3 minutes above 6,500 feet (2,000 m) of altitude) will decontaminate it. Heating milk at 71.7 °C (161 °F) for 15 seconds pasteurizes it and can destroy the oocysts' ability to infect. Water can also be made safe by filtering with a filter with pore size not greater than 1 micrometre, or by filters that have been approved for “cyst removal†by NSF International National Sanitation Foundation. Bottled drinking water is less likely to contain Cryptosporidium, especially if the water is from an underground source.
People with cryptosporidiosis should not swim in communal areas because the pathogen can reside in the anal and genital areas and be washed off. They should wait until at least two weeks after diarrhea stops before entering public water sources, since oocysts can still be shed for a while. Also, they should stay away from immunosuppressed people. Immunocompromised people should take care to protect themselves from water in lakes and streams. They should also stay away from animal stools and wash their hands after touching animals. To be safe, they should boil or filter their water. They should also wash and cook their vegetables.
The US CDC notes the recommendation of many public health departments to soak contaminated surfaces for 20 minutes with a 3% hydrogen peroxide (99% kill rate) and then rinse them thoroughly, with the caveat that no disinfectant is guaranteed to be completely effective against Cryptosporidium. However, hydrogen peroxide is more effective than standard bleach solutions.
Treatment

There is no reliable treatment for cryptosporidium enteritis; certain agents such as paromomycin, atovaquone, nitazoxanide, and azithromycin are sometimes used, but they usually have only temporary effects.
Treatment is primarily supportive. Fluids need to be replaced orally. A lactose-free diet should be taken as tolerated "Cryptosporidiosis Treatment - MedScape". Retrieved October 29, 2013. . In rare situations, intravenous fluids may be required. Antibiotics are not usually helpful, and are reserved primarily for persons with severe disease and a weak immune system. Sometimes relapses happen.
Immunocompetent
The majority of immunocompetent individuals suffer a short (less than 2 weeks) self-limiting course that requires supportive care with rehydration and occasionally antidiarrhoeal medication, and ends with spontaneous recovery. Nitazoxanide is one drug that the US FDA has approved for use in immunocompetent people to combat diarrhea. Spiramycin can help shorten the amount of time oocysts are passed, as well as the duration of diarrhoea in children.
Immunocompromised
In immunocompromised individuals, such as AIDS patients, cryptosporidiosis resolves slowly or not at all, and frequently causes a particularly severe and permanent form of watery diarrhea coupled with a greatly decreased ability to absorb key nutrients through the intestinal tract. The result is progressively severe dehydration, electrolyte imbalances, malnutrition, wasting, and eventual death. Spiramycin can help treat diarrhea in patients in the early stages of AIDS. In general, the mortality rate for infected AIDS patients is based on CD4+ marker counts; in general, patients with CD4+ counts over 180 cells/mm³ recover with supportive hospital care and medication, but, in patients with CD4+ counts below 50 cells/mm³, the effects are usually fatal within three to six months. During the Milwaukee cryptosporidiosis epidemic (the largest of its kind), 73% of AIDS patients with CD4+ counts lower than 50 cells/mm³ and 36% of those with counts between 50 and 200 cells/mm³ died within the first year of contracting the infection. In one AIDS patient from Iran, who had pulmonary cryptosporidiosis in addition to intestinal cryptosporidiosis, azithromycin and paromomycin helped to clear the infection.
Currently, the best approach is to improve the immune status in immunodeficient individuals, which causes the diarrhea to resolve itself in most cases. Biliar drainage may be needed in case the biliary tract is affected.
Currently, research is being done in molecular-based immunotherapy. For example, synthetic isoflavone derivates have been shown to fight off Cryptosporidium parvum in vitro and in a gerbil. Derivates of nitazoxanide, which are synthetic nitro- or nonnitrothiazolide compounds, have also shown promising results in vitro.
Epidemiology

Cryptosporidiosis is found worldwide. It causes 50.8% of water-borne diseases that are attributed to parasites. In developing countries, 8-19% of diarrheal diseases can be attributed to Cryptosporidium. Ten percent of the population in developing countries excretes oocysts. In developed countries, the number is lower at 1â€"3%. The age group most affected is children from 1 to 9 years old.
As of 2010 it caused about 100,000 deaths down from 220,000 in 1990.
Statistics for the United States â€" number of cases:
History
The organism was first described in 1907 by Tyzzer, who recognised it was a coccidian.
Research
A recombinant Cryptosporidium parvum oocyst surface protein (rCP15/60) vaccine has produced an antibody response in a large group of cows and also antibody response in calves fed rCP15/60-immune colostrum produced by these vaccinated cows . This is very promising. Human Cryptosporidium parvum infections are particularly prevalent and often fatal in neonates in developing countries and to immunocompromised people, such as AIDs patients. To date (2013), there is no commercially available effective vaccine against Cryptosporidium parvum, although passive immunization utilizing different zoite surface (glyco)proteins has showed promise. Developmental stages within the life cycle of the parasite that might act as possible targets for vaccine development. The organism is detected in 65-97% of the surface-water supply in the United States and is resistant to most disinfectants used for treatment of drinking water. Antibodies in the serum of humans and animals infected with Cryptosporidium parvum react with several antigens, one of which is a 15 kDa protein (CP15) located on the surface of the organism. This protein is a good candidate for use as a molecular vaccine because previous studies have shown that a monoclonal antibody to CP15 confers passive immunityto mice. Currently, there is no drug therapy or vaccine that is effective against Cryptosporidium parvum.
Other animals
The most important zoonotic reservoirs are cattle, sheep and goats. In addition, in recent years, cryptosporidiosis has plagued many commercial leopard gecko breeders. Several species of the Cryptosporidium family (C. serpentes and others) are involved, and outside of geckos it has been found in monitor lizards, iguanas and tortoises, as well as several snake species.
Notable cases
- In 1987, 13,000 people in Carrollton, Georgia, United States, became ill with cryptosporidiosis. This was the first report of its spread through a municipal water system that met all state and federal drinking water standards.
- In 1993, a waterborne cryptosporidiosis outbreak occurred in Milwaukee, Wisconsin, USA. An estimated 403,000 people became ill, including 4,400 people hospitalized. An estimated 69 people died during the outbreak, according to the CDC.
- The UK's biggest outbreak occurred in Torbay in Devon in 1995.
- In the summer of 1996, Cryptosporidium affected approximately 2,000 people in Cranbrook, British Columbia, Canada. Weeks later, a separate incident occurred in Kelowna, British Columbia, where 10,000 to 15,000 people got sick.
- In April 2001, an outbreak occurred in the city of North Battleford, Saskatchewan, Canada. Between 5800 and 7100 people suffered from diarrheal illness, and 1907 cases of cryptosporidiosis were confirmed. Equipment failures at the city's antiquated water filtration plant following maintenance were found to have caused the outbreak.
- In the summer of 2005, after numerous reports by patrons of gastrointestinal upset, a water park at Seneca Lake State Park, in the Finger Lakes region of upstate New York, USA was found to have two water storage tanks infected with Cryptosporidium. By early September 2005, over 3,800 people reported symptoms of a Cryptosporidium infection. The "Sprayground" was ordered closed for the season on 15 August.
- In October 2005, the Gwynedd and Anglesey areas of North Wales, United Kingdom, suffered an outbreak of cryptosporidiosis. The outbreak may have been linked to the drinking water supply from Llyn Cwellyn, but this is not yet confirmed. As a result, 231 people fell ill and the company Welsh Water (Dwr Cymru) advised 61,000 people to boil their water before use.
- In March 2007, a suspected outbreak occurred in Galway, Ireland, after the source of water for much of the county, Lough Corrib, was suspected to be contaminated with the parasite. A large population (90,000 people), including areas of both Galway City and County, were advised to boil water for drinking, food preparation and for brushing teeth. On 21 March 2007, it was confirmed that the city and county's water supply was contaminated with the parasite. The area's water supply was finally given approval on 20 August 2007, five months after Cryptosporidium was first detected. Around 240 people are known to have contracted the disease; experts say the true figure could be up to 5,000.
- Hundreds of public pools in 20 Utah, USA counties were closed to young children in 2007, as children under 5 are most likely to spread the disease, especially children wearing diapers. As of 10 September 2007 the Utah Department of Health had reported 1302 cases of cryptosporidiosis in the year; a more usual number would be 30. On 25 September the pools were reopened to those not requiring diapers, but hyperchlorination requirements were not lifted.
- On 21 September 2007, a Cryptosporidium outbreak attacked the Western United States: 230 Idaho residents, with hundreds across the Rocky Mountain area; in the Boise and Meridian areas; Utah, 1,600 illnesses; Colorado and other Western states â€" Montana, decrease.
- On 25 June 2008, Cryptosporidium was found in England in water supplies in Northampton, Daventry, and some surrounding areas supplied from the Pitsford Reservoir, as reported on the BBC. People in the affected areas were warned not to drink tap water unless it had been boiled. Anglian Water confirmed that 108,000 households were affected, about 250,000 people. They advised that water might not be fit for human consumption for many weeks. The boil notice was lifted for all the affected customers on 4 July 2008.
- Throughout the summer of 2008; many public swimming areas, water parks, and public pools in the Dallas/Fort Worth Metroplex of Texas, USA suffered an outbreak of cryptosporidiosis. Burger's Lake in Fort Worth was the first to report such an outbreak. This prompted some, if not all, city-owned and private pools to close and hyperchlorinate. To date, there have been 400 reported cases of Cryptosporidium.
- In September 2008, a gym in Cambridge, United Kingdom, was forced to close its swimming pool until further notice after health inspectors found an outbreak of cryptosporidiosis. Environmental Health authorities requested that the water be tested after it was confirmed that a young man had been infected.
- In May 2010, the Behana creek water supply south of Cairns, Australia, was found to be contaminated by cryptosporidium.
- In July 2010, a local sport centre in Cumbernauld (Glasgow, UK) detected traces of cryptosporidium in its swimming pools, causing a temporarily closure of the swimming pools.
- In November 2010, over 4000 cases of cryptosporidiosis were reported in Östersund, Sweden. The source of contamination was the tap water. In mid December 2010 the number of reported cases was 12,400 according to local media.
- As of April 2011, there has been an ongoing outbreak in Skellefteå, Sweden. Although many people have been diagnosed with cryptosporidiosis, the source of the parasite has not yet been found. Several tests have been taken around the water treatment unit "Abborren", but so far no results have turned up positive. Residents are being advised to boil the tap water as they continue to search for the contaminating source.
- Since May 2011, there has been an ongoing outbreak in South Roscommon in Ireland. Although many people have been diagnosed with cryptosporidiosis, the source of the parasite has not yet been found. Testing continues and Roscommon County Council are now considering introducing Ultra Violet Filtration to their water treatment process in the next 12 months. Residents are being advised to boil the tap water and there is no sign of this boil notice being lifted in the near future.
- On May 15, 2013, in Roscommon, Ireland, another outbreak of the cryptosporidiosis was reported and a boil water notice was issued. This was the second time the parasite was detected in a month in the Roscommon water supply. The source of one of the outbreaks had been linked to the agricultural community. To date, 13 people have been treated for Cryptosporidiosis and the boil water notice is still in effect.





0 comments:
Post a Comment