
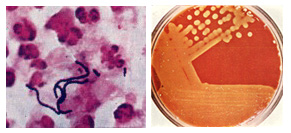
Streptococcus pyogenes is a spherical, gram-positive bacterium that is the cause of group A streptococcal infections. S. pyogenes displays streptococcal group A antigen on its cell wall and typically produces large zones of beta-hemolysis (the complete disruption of erythrocytes and the release of hemoglobin) when cultured on blood agar plates, and is therefore also called group A (beta-hemolytic) Streptococcus (GABHS or GAS).
Streptococci are catalase-negative. Under ideal conditions, S. pyogenes has an incubation period around 1â€"3 days. It is an infrequent, but usually pathogenic, part of the skin flora.
An estimated 700 million infections occur worldwide each year, and over 650,000 cases of severe, invasive infections have a mortality rate of 25%. Early recognition and treatment are critical; diagnostic failure can result in sepsis and death.
Serotyping

In 1928, Rebecca Lancefield published a method for serotyping S. pyogenes based on its M protein, a virulence factor displayed on its surface. Later, in 1946, Lancefield described the serologic classification of S. pyogenes isolates based on their surface T antigen. Four of the 20 T antigens have been revealed to be pili, which are used by bacteria to attach to host cells. Over 220 M serotypes and about 20 T serotypes are known.
Pathogenesis
S. pyogenes is the cause of many important human diseases, ranging from mild superficial skin infections to life-threatening systemic diseases. Infections typically begin in the throat or skin. The most striking sign is a strawberry-like rash. Examples of mild S. pyogenes infections include pharyngitis (strep throat) and localized skin infection (impetigo). Erysipelas and cellulitis are characterized by multiplication and lateral spread of S. pyogenes in deep layers of the skin. S. pyogenes invasion and multiplication in the fascia can lead to necrotizing fasciitis, a life-threatening condition requiring surgery.
Infections due to certain strains of S. pyogenes can be associated with the release of bacterial toxins. Throat infections associated with release of certain toxins lead to scarlet fever. Other toxigenic S. pyogenes infections may lead to streptococcal toxic shock syndrome, which can be life-threatening.
S. pyogenes can also cause disease in the form of postinfectious "nonpyogenic" (not associated with local bacterial multiplication and pus formation) syndromes. These autoimmune-mediated complications follow a small percentage of infections and include rheumatic fever and acute postinfectious glomerulonephritis. Both conditions appear several weeks following the initial streptococcal infection. Rheumatic fever is characterised by inflammation of the joints and/or heart following an episode of streptococcal pharyngitis. Acute glomerulonephritis, inflammation of the renal glomerulus, can follow streptococcal pharyngitis or skin infection.
This bacterium remains acutely sensitive to penicillin. Failure of treatment with penicillin is generally attributed to other local commensal organisms producing β-lactamase, or failure to achieve adequate tissue levels in the pharynx. Certain strains have developed resistance to macrolides, tetracyclines, and clindamycin.
Virulence factors

S. pyogenes has several virulence factors that enable it to attach to host tissues, evade the immune response, and spread by penetrating host tissue layers. A carbohydrate-based bacterial capsule composed of hyaluronic acid surrounds the bacterium, protecting it from phagocytosis by neutrophils. In addition, the capsule and several factors embedded in the cell wall, including M protein, lipoteichoic acid, and protein F (SfbI) facilitate attachment to various host cells. M protein also inhibits opsonization by the alternative complement pathway by binding to host complement regulators. The M protein found on some serotypes is also able to prevent opsonization by binding to fibrinogen. However, the M protein is also the weakest point in this pathogen's defense, as antibodies produced by the immune system against M protein target the bacteria for engulfment by phagocytes. M proteins are unique to each strain, and identification can be used clinically to confirm the strain causing an infection.
Diagnosis
Usually, a throat swab is taken to the laboratory for testing. A Gram stain is performed to show gram-positive cocci in chains. Then, the organism is cultured on blood agar with an added bacitracin antibiotic disk to show beta-hemolytic colonies and sensitivity (zone of inhibition around the disk) for the antibiotic. Culture on agar not containing blood, and then performing the catalase test should show a negative reaction for all streptococci. S. pyogenes is CAMP and hippurate tests negative. Serological identification of the organism involves testing for the presence of group-A-specific polysaccharide in the bacterium's cell wall using the Phadebact test.
Treatment

Thoroughly washing of hands can be the simplest preventive measure. In addition, avoid sharing personal items and practice good hygiene. The treatment of choice is penicillin, and the duration of treatment is well established as being 10 days minimum. No instance of penicillin resistance has been reported to date, although since 1985, many reports of penicillin tolerance have been made.
Macrolides, chloramphenicol, and tetracyclines may be used if the strain isolated has been shown to be sensitive, but resistance is much more common.
Prevention

No vaccines are currently available to protect against S. pyogenes infection, although research has been conducted into the development of one. Difficulties in developing a vaccine include the wide variety of strains of S. pyogenes present in the environment and the large amount of time and people that will be needed for appropriate trials for safety and efficacy of the vaccine.
Applying in bionanotechnology
Many S. pyogenes proteins have unique properties, which have been harnessed in recent years to produce a highly specific "superglue" and a route to enhance the effectiveness of antibody therapy.
Genome

Genome of different strains were sequenced (genome size is 1.8-1.9M bp)






My little princess is so beautiful) I underwent using Dr Itua Herbal Medicine. I had a miscarriage 7 years ago. I still can’t hold back my tears when I remember that horrible period of my life. After my loss I couldn’t get back to life for a long time. I’m glad I have my husband. He gave me support I needed the most. Together we can do everything! We wanted to have kids for a really long time. We’ve gone through a lot, but if you want something badly, you’ll get it! I had to search online on how i can use herbal remedy due to my infertility then i came across Dr Itua how he cure all kind diseases and helped a lady from Kansas City to get pregnant so i contacted him on email,He gave me some guild lines to follow he also send me his herbal medicine via courier service which he instruct me on how to drink it for two weeks really i did and after 7 days of having intercourse with my husband few days later i noticed my period didn't come then i decided to go for check up i was pregnant with a baby,Dr Itua is a genuine miracle man..I've got pregnant from first attempt. We were over the moon! Our girls were born in May 2015. We've just celebrated their first birthday. Finally joy and peace came to our family.Here his Email/Whatsapp Number...+2348149277967/ drituaherbalcenter@gmail.com He cure the following...infertility Liver/kidney Inflammatory,Diabetis,Herpes Virus, Lupus, HPV, Cancer, Hiv/Aids, Hepatitis, Als, MS, Menstrual Cramp, Fribroid.
ReplyDelete