
Cardiovascular disease (also called heart disease) is a class of diseases that involve the heart, the blood vessels (arteries, capillaries, and veins) or both.
Cardiovascular disease refers to any disease that affects the cardiovascular system, principally cardiac disease, vascular diseases of the brain and kidney, and peripheral arterial disease. The causes of cardiovascular disease are diverse but atherosclerosis and hypertension are the most common. In addition, with aging come a number of physiological and morphological changes that alter cardiovascular function and lead to increased risk of cardiovascular disease, even in healthy asymptomatic individuals.
Cardiovascular disease is the leading cause of deaths worldwide, though, since the 1970s, cardiovascular mortality rates have declined in many high-income countries. At the same time, cardiovascular deaths and disease have increased at a fast rate in low- and middle-income countries. Although cardiovascular disease usually affects older adults, the antecedents of cardiovascular disease, notably atherosclerosis, begin in early life, making primary prevention efforts necessary from childhood. There is therefore increased emphasis on preventing atherosclerosis by modifying risk factors, for example by healthy eating, exercise, and avoidance of smoking tobacco.
Types

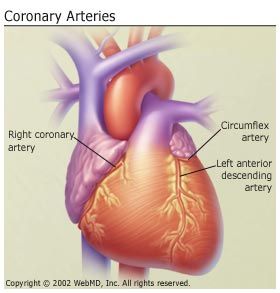
- Coronary artery disease (also known as coronary heart disease and ischemic heart disease)
- Cardiomyopathy â€" diseases of cardiac muscle
- Hypertensive heart disease â€" diseases of the heart secondary to high blood pressure
- Heart failure
- Pulmonary heart disease â€" a failure at the right side of the heart with respiratory system involvement
- Cardiac dysrhythmias â€" abnormalities of heart rhythm
- Inflammatory heart disease
- Endocarditis â€" inflammation of the inner layer of the heart, the endocardium. The structures most commonly involved are the heart valves.
- Inflammatory cardiomegaly
- Myocarditis â€" inflammation of the myocardium, the muscular part of the heart.
- Valvular heart disease
- Cerebrovascular disease â€" disease of blood vessels that supply blood to the brain such as stroke
- Peripheral arterial disease â€" disease of blood vessels that supply blood to the arms and legs
- Congenital heart disease â€" heart structure malformations existing at birth
- Rheumatic heart disease â€" heart muscles and valves damage due to rheumatic fever caused by Streptococcus pyogenes a group A streptococcal infection.
Risk factors

Evidence suggests a number of risk factors for heart diseases: age, gender, high blood pressure, hyperlipidemia, diabetes mellitus, tobacco smoking, processed meat consumption, excessive alcohol consumption, sugar consumption, family history, obesity, lack of physical activity, psychosocial factors, and air pollution. While the individual contribution of each risk factor varies between different communities or ethnic groups the consistency of the overall contribution of these risk factors to epidemiological studies is remarkably strong. Some of these risk factors, such as age, gender or family history, are immutable; however, many important cardiovascular risk factors are modifiable by lifestyle change, social change, drug treatment and prevention of Serrano's Cardiac Triad: hypertension, hyperlipidemia, and diabetes.
Age
Age is by far the most important risk factor in developing cardiovascular or heart diseases, with approximately a tripling of risk with each decade of life. It is estimated that 82 percent of people who die of coronary heart disease are 65 and older. At the same time, the risk of stroke doubles every decade after age 55.
Multiple explanations have been proposed to explain why age increases the risk of cardiovascular/heart diseases. One of them is related to serum cholesterol level. In most populations, the serum total cholesterol level increases as age increases. In men, this increase levels off around age 45 to 50 years. In women, the increase continues sharply until age 60 to 65 years.
Aging is also associated with changes in the mechanical and structural properties of the vascular wall, which leads to the loss of arterial elasticity and reduced arterial compliance and may subsequently lead to coronary artery disease.
Sex
Men are at greater risk of heart disease than pre-menopausal women. Once past menopause, it has been argued that a woman's risk is similar to a man's although more recent data from the WHO and UN disputes this. If a female has diabetes, she is more likely to develop heart disease than a male with diabetes.
Among middle-aged people, coronary heart disease is 2 to 5 times more common in men than in women. In a study done by the World Health Organization, sex contributes to approximately 40% of the variation in the sex ratios of coronary heart disease mortality. Another study reports similar results that gender difference explains nearly half of the risk associated with cardiovascular diseases One of the proposed explanations for the gender difference in cardiovascular disease is hormonal difference. Among women, estrogen is the predominant sex hormone. Estrogen may have protective effects through glucose metabolism and hemostatic system, and it may have a direct effect on improving endothelial cell function. The production of estrogen decreases after menopause, and may change the female lipid metabolism toward a more atherogenic form by decreasing the HDL cholesterol level and by increasing LDL and total cholesterol levels. Women who have experienced early menopause, either naturally or because they have had a hysterectomy, are twice as likely to develop heart disease as women of the same age group who have not yet gone through menopause.
Among men and women, there are notable differences in body weight, height, body fat distribution, heart rate, stroke volume, and arterial compliance. In the very elderly, age-related large artery pulsatility and stiffness is more pronounced in women. This may be caused by the smaller body size and arterial dimensions independent of menopause.
Air pollution
Particulate matter has been studied for its short- and long-term exposure effects on cardiovascular disease. Currently, PM2.5 is the major focus, in which gradients are used to determine CVD risk. For every 10 μg/m3 of PM2.5 long-term exposure, there was an estimated 8â€"18% CVD mortality risk. Women had a higher relative risk (RR) (1.42) for PM2.5 induced coronary artery disease than men (0.90) did. Overall, long-term PM exposure increased rate of atherosclerosis and inflammation. In regards to short-term exposure (2 hours), every 25 μg/m3 of PM2.5 resulted in a 48% increase of CVD mortality risk. In addition, after only 5 days of exposure, a rise in systolic (2.8 mmHg) and diastolic (2.7 mmHg) blood pressure occurred for every 10.5 μg/m3 of PM2.5. Other research has implicated PM2.5 in irregular heart rhythm, reduced heart rate variability (decreased vagal tone), and most notably heart failure. PM2.5 is also linked to carotid artery thickening and increased risk of acute myocardial infarction.
Pathophysiology
Population-based studies show that atherosclerosis, the major precursor of cardiovascular disease, begins in childhood. The Pathobiological Determinants of Atherosclerosis in Youth Study demonstrated that intimal lesions appear in all the aortas and more than half of the right coronary arteries of youths aged 7â€"9 years.
This is extremely important considering that 1 in 3 people die from complications attributable to atherosclerosis. In order to stem the tide, education and awareness that cardiovascular disease poses the greatest threat, and measures to prevent or reverse this disease must be taken.
Obesity and diabetes mellitus are often linked to cardiovascular disease, as are a history of chronic kidney disease and hypercholesterolaemia. In fact, cardiovascular disease is the most life-threatening of the diabetic complications and diabetics are two- to four-fold more likely to die of cardiovascular-related causes than nondiabetics.
Screening
Screening ECGs (either at rest or with exercise) are not recommended in those without symptoms who are at low risk. This includes those who are young without risk factors. In those at higher risk the evidence for screening with ECGs is inconclusive.
Some biomarkers may add to conventional cardiovascular risk factors in predicting the risk of future cardiovascular disease; however, the clinical value of some biomarkers is still questionable. Currently, biomarkers that may reflect a higher risk of cardiovascular disease include the following:
- Coronary artery calcification
- Carotid intima-media thickness
- Carotid total plaque area
- Higher fibrinogen and PAI-1 blood concentrations
- Elevated homocysteine
- Elevated blood levels of asymmetric dimethylarginine
- Inflammation as measured by C-reactive protein
- Elevated Low-density lipoprotein-p
- Elevated blood levels of brain natriuretic peptide (also known as B-type) (BNP)
Prevention

Currently practiced measures to prevent cardiovascular disease include:
- A low-fat, high-fiber diet including whole grains and fruit and vegetables. Five portions a day reduces risk by about 25%.
- Tobacco cessation and avoidance of second-hand smoke
- Limit alcohol consumption to the recommended daily limits consumption of 1â€"2 standard alcoholic drinks per day may reduce risk by 30% However excessive alcohol intake increases the risk of cardiovascular disease.
- Lower blood pressures, if elevated
- Decrease body fat if overweight or obese
- Increase daily activity to 30 minutes of vigorous exercise per day at least five times per week (multiply by three if horizontal);
- Reduce sugar consumptions
- Decrease psychosocial stress. Stress however plays a relatively minor role in hypertension (if it even plays any role in the development of hypertension at all is often disputed). Specific relaxation therapies are not supported by the evidence.
For adults without a known diagnosis of hypertension, diabetes, hyperlipidemia, or cardiovascular disease, routine counseling to advise them to improve their diet and increase their physical activity has not been found to significantly alter behavior, and thus is not recommended. It is unclear whether or not dental care in those with periodontitis affects the risk of cardiovascular disease. Exercise in those who at high risk of heart disease has not been well studied as of 2014.
Diet
A diet high in fruits and vegetables decreases the risk of cardiovascular disease and death. Evidence suggests that the Mediterranean diet may improve cardiovascular outcomes. There is also evidence that a Mediterranean diet may be more effective than a low-fat diet in bringing about long-term changes to cardiovascular risk factors (e.g., lower cholesterol level and blood pressure). The DASH diet (high in nuts, fish, fruits and vegetables, and low in sweets, red meat and fat) has been shown to reduce blood pressure, lower total and low density lipoprotein cholesterol and improve metabolic syndrome; but the long term benefits outside the context of a clinical trial have been questioned. A high fiber diet appears to lower the risk.
Total fat intake does not appear to be an important risk factor. A diet high in trans fatty acids; however, does appear to increase rates of cardiovascular disease. Worldwide, dietary guidelines recommend a reduction in saturated fat. However, there are some questions around the effect of saturated fat on cardiovascular disease in the medical literature. A 2014 review did not find evidence of harm from saturated fats. A 2012 Cochrane review found suggestive evidence of a small benefit from replacing dietary saturated fat by unsaturated fat. A 2013 meta analysis concludes that substitution with omega 6 linoleic acid (a type of unsaturated fat) may increase cardiovascular risk. Replacement of saturated fats with carbohydrates does not change or may increase risk. Benefits from replacement with polyunsaturated fat appears greatest however supplementation with omega-3 fatty acids (a type of polysaturated fat) does not appear have an effect.
The effect of a low-salt diet is unclear. A Cochrane review concluded that any benefit in either hypertensive or normal-tensive people is small if present. In addition, the review suggested that a low-salt diet may be harmful in those with congestive heart failure. However, the review was criticized in particular for not excluding a trial in heart failure where people had low-salt and -water levels due to diuretics. When this study is left out, the rest of the trials show a trend to benefit. Another review of dietary salt concluded that there is strong evidence that high dietary salt intake increases blood pressure and worsens hypertension, and that it increases the number of cardiovascular disease events; the latter happen both through the increased blood pressure and, quite likely, through other mechanisms. Moderate evidence was found that high salt intake increases cardiovascular mortality; and some evidence was found for an increase in overall mortality, strokes, and left ventricular hypertrophy.
Supplements
While a healthy diet is beneficial, in general the effect of antioxidant supplementation (vitamin E, vitamin C, etc.) or vitamins has not been shown to protection against cardiovascular disease and in some cases may possibly result in harm. Mineral supplements have also not been found to be useful. Niacin, a type of vitamin B3, may be an exception with a modest decrease in the risk of cardiovascular events in those at high risk. Magnesium supplementation lowers high blood pressure in a dose dependent manner. Magnesium therapy is recommended for patients with ventricular arrhythmia associated with torsade de pointes who present with long QT syndrome as well as for the treatment of patients with digoxin intoxication-induced arrhythmias. Evidence to support omega-3 fatty acid supplementation is lacking.
Medication
Aspirin has been found to be of benefit overall in those at low risk of heart disease as the risk of serious bleeding is equal to the benefit with respect to cardiovascular problems.
Statins are effective in preventing further cardiovascular disease in people with a history of cardiovascular disease. As the event rate is higher in men than in women, the decrease in events is more easily seen in men than women. In those without cardiovascular disease but risk factors statins appear to also be beneficial with a decrease in mortality and further heart disease. The time course over which statins provide preventation against death appears to be long, of the order of one year, which is much longer than the duration of their effect on lipids. The medications niacin, fibrates and CETP Inhibitors, while they may increase HDL cholesterol do not affect the risk of cardiovascular disease in those who are already on statins.
Management
Cardiovascular disease is treatable with initial treatment primarily focused on diet and lifestyle interventions.
Epidemiology

Cardiovascular diseases are the leading cause of death. In 2008, 30% of all global death is attributed to cardiovascular diseases. Death caused by cardiovascular diseases are also higher in low- and middle-income countries as over 80% of all global death caused by cardiovascular diseases occurred in those countries. It is also estimated that by 2030, over 23 million people will die from cardiovascular diseases each year.
Research

The first studies on cardiovascular health were performed in year 1949 by Jerry Morris using occupational health data and were published in year 1958. The causes, prevention, and/or treatment of all forms of cardiovascular disease remain active fields of biomedical research, with hundreds of scientific studies being published on a weekly basis.
A fairly recent emphasis is on the link between low-grade inflammation that hallmarks atherosclerosis and its possible interventions. C-reactive protein (CRP) is a common inflammatory marker that has been found to be present in increased levels in patients who are at risk for cardiovascular disease. Also osteoprotegerin, which is involved with regulation of a key inflammatory transcription factor called NF-κB, has been found to be a risk factor of cardiovascular disease and mortality.
Some areas currently being researched include the possible links between infection with Chlamydophila pneumoniae (a major cause of pneumonia) and coronary artery disease. The Chlamydia link has become less plausible with the absence of improvement after antibiotic use.
Several research also investigated the benefits of melatonin on cardiovascular diseases prevention and cure. Melatonin is a pineal gland secretion and it is shown to be able to lower total cholesterol, very-low-density and low-density lipoprotein cholesterol levels in the blood plasma of rats. Reduction of blood pressure is also observed when pharmacological doses are applied. Thus, it is deemed to be a plausible treatment for hypertension. However, further research needs to be conducted to investigate the side-effects, optimal dosage, etc. before it can be licensed for use.
References
External links
- Cardiovascular disease at DMOZ
- European Guidelines on cardiovascular disease prevention in clinical practice (version 2012)





My Husband have been suffering from Ischemic heart disease 15 years with no success. our doctor told me that only surgery can solve it, I didn't want my husband to go for any surgery, so I searched the Internet for natural treatments for Ischemic heart disease. I found a contact of a Doctor and looked at all the testimonials, everything looked good so I ordered for the medication,
ReplyDeleteIt arrived very quickly and I began to take it. Within 2 months of taking them,I was cured, I am glad. contact the doctor at, drbenson833@gmail.com. also for a good solution.
Wonderful article! We are linking to this great post on our site. Keep up the good writing.
ReplyDeletecardiovascular disease
Thank you for sharing such wonderful information! When it comes to health, there is nothing more important than managing to eat healthy food and doing exercise regularly.
ReplyDeleteHealth Jobs Australia
ALL THANKS TO DR JOHNSON WITH HIS HERB I WAS CURED FROM A TERRIBLE HEART DISEASE (Cardiovascular Disease)
ReplyDeleteIs my pleasure to comment on this site and I thank the admin of this site
for his/her great work so far.
I really don’t know how to thank DR Johnson
for helping me my Husband get cured for over 5 year of suffering from a
terrible Heart Disease(Cardiovascular), His Illness started when He was 55 year I thought is going to end one day but even get worse as days went by,i have tried all western drugs prescribed by doctors but to no avail I lost total concentration,I
came across DR Johnson contact through a headline news on internet about
how DR Johnson have help so many people to get cured of various Heart Diseases, and so many other with similar body problem I contacted him and he told me how to get his herb,few day later he sent me the herbal portion which my husband too
every morning for One Month and his medicine was able to restore my husband back to normal and now he is very okay without any side effects whatsoever If you have any Heart problem you can contact him on his email address drjohnson958@gmail.com
I'm a living testimony of Dr Okosun musa he help me cured my heart disease within 1 month and two weeks with his herbal medicine without sugary he can help you too contact him on his email drokosunmusa@gmail.com or you can call or whatsapp him on +233551428414 or +2349056175191 whatsapp only
ReplyDeleteMY DAUGHTER CANCER HEALING TESTIMONEY
ReplyDeleteHi everyone, this is good news, a perfect and greats one. My daughter of
17years who has suffered of Colon Cancer Stage for 2 and half years has been
cure by a Herbal doctor called Dr voodoo, who uses herbal and traditional
medicine to cure people. I have spent so much on my daughter's health for
years but no improvement. A friend told me about this herbal man who cure
people with herbal medicine. he cures all sickness, diseases, viruses, and
infections with his different herbal curing medicine.The result that
declares my daughter janet healed was from a hospital here in USA, And the
results of the test says my daughter was okay. Dr voodoo directed that
janet would be heal in 7days if she uses the medicine as directed. And
7days later, we went to confirm from the central hospital and several test
that was done says my daughter is not sick or anything. So she was cured by
this herbal doctor in 7days. This amaze me though. I would advice everyone
to meet this Dr voodoo his email is voodoospelltemple66@gmail.com
for his herbal medicine to cure your illness because am happy to see my
daughter healthy again.Meet Dr voodoo and set yourself and your love ones
will free you can also add Dr voodoo on whatsApp +2348140120719