
Cyclospora cayetanensis is a protozoan that causes disease in humans, and perhaps primates. It has been linked in the United States to fecally contaminated imported raspberries and was virtually unknown before about 1990, but has been on the rise since. The health risk associated with the disease is usually confined to adult foreigners visiting regions where the species is endemic and acquiring the infection, which is why C. cayetanensis has been labeled as causing "traveler's diarrhea."
This species was placed in the Cyclospora genus because of the spherical shape of its sporocysts. The species name refers to the Cayetano Heredia University in Lima, Peru, where early epidemiological and taxonomic work was done.
Characterization
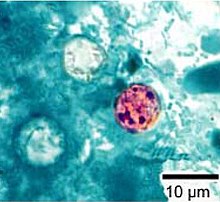
Cyclospora cayetanensis is an apicomplexan, cyst-forming coccidian protozoan that causes a self-limiting diarrhea. In terms of morphology, C. cayetanensis has spherical oocysts that are between 7.5 and 10 micrometers in diameter that also have a 50-nanometer-thick wall with an outer threadlike coat that has been called a wrinkle by some researchers.
The only hosts for C. cayentanensis are humans. The protozoan lives out its lifecycle intracellularly within the host’s epithelial cells and gastrointestinal tract. Infection is transmitted through the fecal-oral route, and begins when a person ingests oocysts in fecally contaminated food or water. Various chemicals in the host's gastrointestinal tract cause the oocysts to excyst and release sporozoites; generally, two are observed per oocyst. After these sporozoites invade the epithelial cells, they undergo merogony, a form of asexual reproduction that results in many daughter merozoites. These daughter cells may either infect new host cells and initiate yet another round of merogony or take on a sexual track via gametogony: Daughter merozoites become male macrogamonts â€" which form many microgametes â€" and female macrogamonts. After fertilization has occurred via male microgamete fusion with female macrogamont, the zygote matures into an oocyst and ruptures the host cell, from which point it is passed with the stool. The oocysts that are passed are not, however, immediately infectious. Sporulation can take from one to several weeks, meaning person-to-person transmission is not a likely problem. This differentiates C. cayentanensis from Cryptosporidium parvum â€" a closely related organism that causes a similar disease â€" since C. parvum oocysts are immediately infectious upon release from the host.
Symptoms

C. cayentanensis causes gastroenteritis, with the extent of the illness varying based on age, condition of the host, and size of the infectious dose. Symptoms include "watery diarrhea, loss of appetite, weight loss, abdominal bloating and cramping, increased flatulence, nausea, fatigue, and low-grade fever", though this can be augmented in more severe cases by vomiting, substantial weight loss, excessive diarrhea, and muscle aches. Typically, patients with a persistent watery diarrhea lasting over several days may be suspected of harboring the disease, especially if they have traveled to a region where the protozoan is endemic. The incubation period in the host is typically around a week, and illness can last six weeks before self-limiting. Unless treated, illness may relapse. The more severe forms of the disease can occur in immunocompromised patients, such as those with AIDS.
Recognition
Due to its small size, intracellular habitat, and inability to properly take up many histological stains, diagnosis of C. cayetanensis can be very difficult. Four methods have thus far been established for positive diagnosis of the protozoan: microscopic detection in stool samples of oocysts; recovering oocysts in intestinal fluid/small bowel biopsy specimens; demonstration of oocyst sporulation; and amplification by polymerase chain reaction (PCR) of C. cayetanensis DNA. Since detection is so hard, one negative result should not discount the possibility of C. cayetanensis: tests involving fresh stool samples over the next few days should also be considered.
Except for PCR amplification, once a sample with suspected oocysts has been recovered, standard tests are followed to identify C. cayetanensis. These tests include phase contrast microscopy to check for the spherical oocysts described earlier, modified acid-fast staining to check for variable staining (from pale to red), and autofluorescence with UV lights. Obtaining these oocysts is usually the challenge, though recent studies show easier methods of obtaining them. In a recent study on different techniques used in fecal exams to identify oocysts, centrifuging a sample of feces in a sucrose solution and then transferring a small amount to a slide was found to be remarkably effective â€" both in oocysts found and relative ease of labor â€" in detecting C. cayetanensis oocysts: indeed, the paper concluded the positive samples obtained were around 84%.
C. cayetanensis has been confused with other protozoan infections in the past, most commonly being misidentified as Cryptosporidium parvum. Several differences can be noted between the two, however, to ensure proper diagnosis. These differences include: size difference â€" C. parvum is smaller; differing results from modified acid-fast staining â€" C. parvum has consistent red staining, whereas C. cayetanensis shows variable staining; and autofluorescence under UV light â€" C. cayetanensis exhibits this, whereas C. parvum does not.
Treatment
Though the diarrhea caused by C. cayetanensis is self-limiting, relapses can and do occur. To date, the most effective drug for the treatment of the protozoan is a seven-day course of oral trimethoprim-sulfamethoxazole (TMP-SMX). Effects of the drug include a significant decrease in the duration of oocyst excretion, cessation of diarrhea, and stool samples negative for oocysts within two to three days. Relapses respond promptly to therapy, and using TMP-SMX as a prophylaxis for HIV/AIDS patients and immunocompromised patients (ex: organ transplant recipients) has been mentioned.
Prevention
Since infection occurs via fecally contaminated food and water in endemic environments, several simple solutions have been suggested for the prevention of C. cayetanensis infections. The simplest one is to warn travelers not to visit regions where the protozoan is endemic (in general, tropical and subtropical regions where sanitation is poor, such as Peru, Brazil, and Haiti), especially when the disease is in its best season for spreading: Such was the reason behind the first reported case of cyclosporiasis in Korea. This is not to say that natives of a region are completely free from possible infection: A middle-age Turkish lawyer living in an urban area with water sanitized by the local government and with no travel history recently became Turkey’s first autochthonous case. This woman is presumed to have received the infection from consuming some infected foodstuffs (possibly raspberries) that were not thoroughly washed before consumption. Thus, better health practices in the originating agricultural setting â€" such as ensuring produce is fully washed and kept away from human feces â€" and in the individual's environmentâ€"taking an extra few seconds to wash that produce as well â€" would lead to a lower incidence of infection.
2013 United States outbreak

At least 285 people in 11 states have been affected as of July 26, 2013. The exact cause of the outbreak has not yet been identified according to the U.S. Centers for Disease Control and Prevention (CDC). The majority of cases are located in the Midwest, with 138 reported cases in Iowa and 70 in Nebraska. The other states affected are: Texas, Florida, Georgia, Wisconsin, Connecticut, Illinois, Kansas, Minnesota, New Jersey, and Ohio.
As of July 29, 2013, the CDC reported 373 people in 15 states have been affected by the outbreak. So far, 21 patients from three states have been hospitalized, but no deaths have been reported. No food source has been identified yet, but health officials in Iowaâ€"the state reporting the most casesâ€"have said they suspect imported vegetables.
On July 30, 2013, the Nebraska Department of Health & Human Services and the Iowa Department of Health announced that a restaurant chain's prepackaged salad was the disease vector for the parasite. However, the CDC and the U.S. Food and Drug Administration (FDA) are still assessing information from other states to see if the findings apply to illnesses there.
In an August 1, 2013, update, the CDC reported 397 cases, while and Iowa and Texas added another 22 more. This pushed the unofficial count to over 400 cases. Additionally, Louisiana reported its first case, bringing the total number of states affected to 16.
On August 3, 2013, CNN reported that the outbreak was traced to prepackaged salad served at Olive Garden and Red Lobster restaurants that were manufactured by Taylor Farms de Mexico.
On August 15, 2013, the CDC reported nine more Cyclospora infections, raising its case count to 548. The number of affected states remained at 19, but the CDC said that not all cases are confirmed to be linked to an outbreak in Iowa and Nebraska traced to a contaminated salad mix from Mexico.
On August 19, 2013, the CDC reported 10 more Cyclospora cases, raising the unofficial count to over 600. Tennessee also reported its first case, bringing the number of states affect to 20. The CDC still cautions that it is not clear whether cases in all of the states are related to outbreaks in Iowa and Nebraska.
On August 27, 2013, the origination still remained a mystery. The FDA says it found no food safety violations at the Taylor Farms de Mexico salad plant in Mexico that was linked to some of the illnesses.
References
- Türk M, Türker M, Ak M, Karaayak B, Kaya T (March 2004). "Cyclosporiasis associated with diarrhoea in an immunocompetent patient in Turkey". J. Med. Microbiol. 53 (Pt 3): 255â€"7. doi:10.1099/jmm.0.45531-0. PMID 14970253.Â
- Kimura K, Kumar Rai S, Takemasa K, et al. (September 2004). "Comparison of three microscopic techniques for diagnosis of Cyclospora cayentanensis". FEMS Microbiol. Lett. 238 (1): 263â€"6. doi:10.1016/j.femsle.2004.07.045. PMID 15336431.Â
- Mansfield LS, Gajadhar AA (December 2004). "Cyclospora cayentanensis, a food- and waterborne coccidian parasite". Vet. Parasitol. 126 (1â€"2): 73â€"90. doi:10.1016/j.vetpar.2004.09.011. PMID 15567580.Â
- Yu JR, Sohn WM (October 2003). "A case of human cyclosporiasis causing traveler's diarrhea after visiting Indonesia". J. Korean Med. Sci. 18 (5): 738â€"41. PMC 3055112. PMID 14555830.Â






0 comments:
Post a Comment