
Hepatocellular carcinoma (HCC, also called malignant hepatoma) is the most common type of liver cancer. Most cases of HCC are secondary to either a viral hepatitis infection (hepatitis B or C) or cirrhosis (alcoholism being the most common cause of hepatic cirrhosis).
Treatment options of HCC and prognosis are dependent on many factors but especially on tumour size and staging. Tumour grade is also important. High-grade tumours will have a poor prognosis, while low-grade tumors may go unnoticed for many years, as is the case in many other organs.
HCC is a relatively uncommon cancer in the United States. In countries where hepatitis is not common, most cancers of the liver are not primary HCC but metastasis (cancers spread from elsewhere in the body such as the colon).
Signs and symptoms

Hepatocellular carcinoma may present with yellow skin, bloating from fluid in the abdomen, easy bruising from blood clotting abnormalities, loss of appetite, unintentional weight loss, abdominal pain especially in the right upper quadrant, nausea, vomiting, or feeling tired.
Risk factors

The main risk factors for hepatocellular carcinoma are;
- Alcoholism
- Hepatitis B
- Hepatitis C (25% of causes globally)
- Aflatoxin
- Cirrhosis of the liver
- Hemochromatosis
- Wilson's disease (while some theorise the risk increases, case studies are rare and suggest the opposite where Wilson's disease actually may confer protection)
- Type 2 diabetes (probably aided by obesity)
The risk factors which are most important varies widely from country to country. In countries where Hepatitis B is endemic, such as China, Hepatitis B will be the predominant cause of Hepatocellular Carcinoma. Whereas in countries, such as the United States, where Hepatitis B is rare because of high vaccination rates, the major cause of HCC is Cirrhosis (often due to alcohol abuse).
The risk of hepatocellular carcinoma in type 2 diabetics is greater (from 2.5 to 7.1 times the non diabetic risk) depending on the duration of diabetes and treatment protocol. A suspected contributor to this increased risk is circulating insulin concentration such that diabetics with poor insulin control or on treatments that elevate their insulin output (both states that contribute to a higher circulating insulin concentration) show far greater risk of hepatocellular carcinoma than diabetics on treatments that reduce circulating insulin concentration. On this note, some diabetics who engage in tight insulin control (by keeping it from being elevated) show risk levels low enough to be indistinguishable from the general population. This phenomenon is thus not isolated to diabetes mellitus type 2 since poor insulin regulation is also found in other conditions such as metabolic syndrome (specifically, when evidence of non alcoholic fatty liver disease or NAFLD is present) and again there is evidence of greater risk here too. While there are claims that anabolic steroid abusers are at greater risk (theorized to be due to insulin and IGF exacerbation), the only evidence that has been confirmed is that anabolic steroid users are more likely to have hepatocellular adenomas (a benign form of HCC) transform into the more dangerous hepatocellular carcinoma.
When hepatocellular adenomas grow to a size of more than 6â€"8 cm, they are considered cancerous and thus become a risk of hepatocellular carcinoma. Although hepatocellular carcinoma most commonly affects adults, children who are affected with biliary atresia, infantile cholestasis, glycogen-storage diseases, and other cirrhotic diseases of the liver are predisposed to developing hepatocellular carcinoma.
Children and adolescents are unlikely to have chronic liver disease, however, if they suffer from congenital liver disorders, this fact increases the chance of developing hepatocellular carcinoma.
Young adults afflicted by the rare fibrolamellar variant of hepatocellular carcinoma may have none of the typical risk factors, i.e. cirrhosis and hepatitis.
Pathogenesis
Hepatocellular carcinoma, like any other cancer, develops when there is a mutation to the cellular machinery that causes the cell to replicate at a higher rate and/or results in the cell avoiding apoptosis. In particular, chronic infections of hepatitis B and/or C can aid the development of hepatocellular carcinoma by repeatedly causing the body's own immune system to attack the liver cells, some of which are infected by the virus, others merely bystanders. While this constant cycle of damage followed by repair can lead to mistakes during repair which in turn lead to carcinogenesis, this hypothesis is more applicable, at present, to hepatitis C. Chronic hepatitis C causes HCC through the stage of cirrhosis. In chronic hepatitis B, however, the integration of the viral genome into infected cells can directly induce a non-cirrhotic liver to develop HCC. Alternatively, repeated consumption of large amounts of ethanol can have a similar effect. Besides, cirrhosis is commonly caused by alcoholism, chronic hepatitis B and chronic hepatitis C. The toxin aflatoxin from certain Aspergillus species of fungus is a carcinogen and aids carcinogenesis of hepatocellular cancer by building up in the liver. The combined high prevalence of rates of aflatoxin and hepatitis B in settings like China and West Africa has led to relatively high rates of heptatocellular carcinoma in these regions. Other viral hepatitides such as hepatitis A have no potential to become a chronic infection and thus are not related to hepatocellular carcinoma.
Diagnosis

Hepatocellular carcinoma (HCC) most commonly appears in a patient with chronic viral hepatitis (hepatitis B or hepatitis C, 20%) or/and with cirrhosis (about 80%). These patients commonly undergo surveillance with ultrasound due to the cost-effectiveness.
Surveillance differs but the American Association of Liver Diseases recommends screening Asian men over the age of 40, Asian women over the age of 50, patients with HBV and cirrhosis, and African and North American blacks. These patients are screened with US every 6 months. AFP is a marker that is useful if it is markedly elevated. At levels less >20 sensitivity is 41-65% and specificity is 80-94%. However at levels >200 sensitivity is 31, specificity is 99%.
Ultrasound (US) is often the first imaging and screening modality used. On US, HCC often appears as a small hypo-echoic lesion with poorly defined margins and coarse irregular internal echoes. When the tumor grows, it can sometimes appear heterogeneous with fibrosis, fatty change, and calcifications. This heterogeneity can look similar to cirrhosis and the surrounding liver parenchyma. A systemic review found that the sensitivity was 60 percent (95% CI 44-76%) and specificity was 97 percent (95% CI 95-98%) compared with pathologic examination of an explanted or resected liver as the reference standard. The sensitivity increases to 79% with AFP correlation.
In patients with a higher suspicion of HCC (such as rising alpha-fetoprotein and des-gamma carboxyprothrombin levels), the best method of diagnosis involves a CT scan of the abdomen using intravenous contrast agent and three-phase scanning (before contrast administration, immediately after contrast administration, and again after a delay) to increase the ability of the radiologist to detect small or subtle tumors. It is important to optimize the parameters of the CT examination, because the underlying liver disease that most HCC patients have can make the findings more difficult to appreciate.
Triple phase helical CT improves the detection of these tumors. Due to the increased vascularity of hepatocellular carcinoma, the classic finding on CT imaging is hypervascularity in the arterial phase with washout in the portal and delayed phases. A pseudocapsule, a mosaic pattern and both calcifications and intralesional fat may be appreciated. A systemic review found that the sensitivity was 68 percent (95% CI 55-80%) and specificity was 93 percent (95% CI 89-96%) compared with pathologic examination of an explanted or resected liver as the reference standard. With triple phase helical CT, the sensitivity 90% or higher, but this data has not been confirmed with autopsy studies.
Classification of HCC on CT: Liver Image Reporting and Data System (LI-RADS): LI-RADs is the new way to standardize/classify the HCC lesions found on CT and MRI. Radiologists use this classification system in their imaging reports in order to further characterize suspicious lesions. As a general introduction, LR1 and LR2 get continued surveillance. LR3 has variable follow up. LR4 gets close follow up, additional imaging or treatment. LR5 gets treatment. See http://www.acr.org/Quality-Safety/Resources/LIRADS for complete details.
On CT, HCC can have three distinct patterns of growth:
- A single large tumor
- Multiple tumors
- Poorly defined tumor with an infiltrative growth pattern
A biopsy is not needed to confirm the diagnosis of HCC if certain imaging criteria are met.
CT scans use contrast agents, which are typically iodine- or barium-based. Some patients are allergic to one or both of these contrast agents, most often iodine. Usually the allergic reaction is manageable and not life-threatening.
An alternative to a CT imaging study would be Magnetic Resonance Imaging (MRI). MRI has about the same sensitivity for detecting HCC has helical CT. However, MRI has the advantage of delivering high resolution images of the liver without nephrotoxic contrast agents or ionizing radiation. HCC appears as a high intensity pattern on T2 weighted images and a low intensity pattern on T1 weighted images. The advantage of MRI is that is has improved sensitivity and specificity when compared to US and CT in cirrhotic patients in whom it can be difficult to differentiate HCC from regenerative nodules. A systematic review found that the sensitivity was 81 percent (95% CI 70-91%) and specificity was 85 percent (95% CI 77-93%) compared with pathologic examination of an explanted or resected liver as the reference standard. The sensitivity is further increased gadoxetic acid-enhanced and diffusion-weighted imaging are combined. Despite the advantages of MRI, helical CT remains the technique of choice among radiologists due to the high cost and long image acquisition time of MRI.
In a review article of the screening, diagnosis and treatment of hepatocellular carcinoma, 4 articles were selected for comparing the accuracy of CT and MRI in diagnosing this malignancy. Radiographic diagnosis was verified against post-transplantation biopsy as the gold standard. With the exception of one instance of specificity, it was discovered that MRI was more sensitive and specific than CT in all four studies.
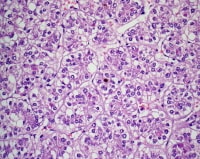
Pathology
Macroscopically, liver cancer appears as a nodular or infiltrative tumor. The nodular type may be solitary (large mass) or multiple (when developed as a complication of cirrhosis). Tumor nodules are round to oval, grey or green (if the tumor produces bile), well circumscribed but not encapsulated. The diffuse type is poorly circumscribed and infiltrates the portal veins, or the hepatic veins (rarely).
Microscopically, there are four architectural and cytological types (patterns) of hepatocellular carcinoma: fibrolamellar, pseudoglandular (adenoid), pleomorphic (giant cell) and clear cell. In well differentiated forms, tumor cells resemble hepatocytes, form trabeculae, cords and nests, and may contain bile pigment in cytoplasm. In poorly differentiated forms, malignant epithelial cells are discohesive, pleomorphic, anaplastic, giant. The tumor has a scant stroma and central necrosis because of the poor vascularization.
Staging
Important features that guide treatment include: -
- size
- spread (stage)
- involvement of liver vessels
- presence of a tumor capsule
- presence of extrahepatic metastases
- presence of daughter nodules
- vascularity of the tumor
MRI is the best imaging method to detect the presence of a tumor capsule.
Prevention

Since hepatitis B or C is one of the main causes of hepatocellular carcinoma, prevention of this infection is key to then prevent hepatocellular carcinoma. Thus, childhood vaccination against hepatitis B may reduce the risk of liver cancer in the future.
In the case of patients with cirrhosis, alcohol consumption is to be avoided. Also, screening for hemochromatosis may be beneficial for some patients.
It is unclear if screening those with chronic liver disease for hepatocellular carcinoma improves outcomes.
Management
- Liver transplantation to replace the diseased liver with a cadaveric liver or a living donor graft has historically low survival rates (20%-36%). During 1996â€"2001 the rate had improved to 61.1%, likely related to adoption of the Milan criteria at US transplantation centers. Expanded Shanghai criteria in China resulted in overall survival and disease-free survival rates similar to the Milan criteria. Studies from the late 2000 obtained higher survival rates ranging from 67% to 91%. If the liver tumor has metastasized, the immuno-suppressant post-transplant drugs decrease the chance of survival. Considering this objective risk in conjunction with the potentially high rate of survival, some recent studies conclude that: "LTx can be a curative approach for patients with advanced HCC without extrahepatic metastasis". For those reasons, and others, it is considered nowadays that patient selection is a major key for success.
- A receptor tyrosine kinase inhibitor, Sorafenib, approved by the US FDA in December 2005 and in Europe in July 2006, may be used in patients with advanced hepatocellular carcinoma. Sorafenib is a small molecule that inhibits tumor-cell proliferation and tumor angionesis. It has been shown in a Spanish phase III clinical trial to add two months to the lifespan of late stage HCC patients with well preserved liver function. It also increases the rate of apoptosis in other tumor models. The results indicated that single-agent sorafenib might have a beneficial therapeutic effect. In this study, for instance, the median overall survival was of 9.2 months and the median time to progression was of 5.5 months. Also, the survival benefit represented a 31% relative reduction in the risk of death.
- Surgical resection to remove a tumor together with surrounding liver tissue while preserving enough liver remnant for normal body function. This treatment offers the best prognosis for long-term survival, but only 10-15% of patients are suitable for surgical resection. This is often because of extensive disease or poor liver function. Resection in cirrhotic patients carries high morbidity and mortality. The expected liver remnant should be more than 25% of the total size for a non-cirrhotic liver, while that should be more than 40% of the total size for a cirrhotic liver. The overall recurrence rate after resection is 50-60%.
Interventional Radiology (IR) Procedures and Management
- Transcatheter arterial chemoembolization (TACE) is usually performed for unresectable tumors or as a temporary treatment while waiting for liver transplant. TACE is done by injecting an antineoplastic drug (e.g. cisplatin) mixed with a radioopaque contrast (e.g. Lipiodol) and an embolic agent (e.g. Gelfoam) into the right or left hepatic artery via the groin artery. The goal of the procedure it to restrict the tumor’s vascular supply while supplying a targeted chemotherapeutic agent. TACE has been shown to increase survival and to downstage HCC in patients who exceed the Milan criteria for liver transplant. Patients who undergo the procedure may are followed with CT scans and may need additional TACE procedures if the tumor persists. As of 2005, multiple trials show objective tumor responses and slowed tumor progression but questionable survival benefit compared to supportive care; greatest benefit seen in patients with preserved liver function, absence of vascular invasion, and smallest tumors. TACE is not suitable for big tumors (>8 cm), presence of portal vein thrombus, tumors with portal-systemic shunt and patients with poor liver function.
- Radiofrequency ablation (RFA) uses high frequency radio-waves to destroy tumor by local heating. The electrodes are inserted into the liver tumor under ultrasound image guidance using percutaneous, laparoscopic or open surgical approach. It is suitable for small tumors (<5 cm). RFA has the best outcomes in patient’s with a solitary tumor less than 4mm. Since it is a local treatment and has minimal affect on normal healthy tissue, it can be repeated multiple times. Survival is better for those with smaller tumors. In one study, In one series of 302 patients, the three-year survival rates for lesions >5 cm, 2.1 to 5 cm, and ≤2 cm were 59, 74, and 91 percent, respectively. A large randomised trial comparing surgical resection and RFA for small HCC showed similar 4 years-survival and less morbidities for patients treated with RFA.
- Selective internal radiation therapy (SIRT) can be used to destroy the tumor from within (thus minimizing exposure to healthy tissue). Similar to TACE, this is a procedure in which an interventional radiologist selectively injects the artery or arteries supplying the tumor with a chemotherapeutic agent. The agent is typically Yttrium-90 (Y-90) incorporated into embolic microspheres that lodge in the tumor vasculature causing ischemia and delivering their radiation dose directly to the lesion. This technique allows for a higher, local dose of radiation to be delivered directly to the tumor while sparing normal healthy tissue. While not curative, patients have increased survival. No studies have been done to compare whether SIRT is superior to TACE in terms of survival outcomes, although retrospective studies suggest similar efficacy. There are currently two products available, SIR-Spheres and TheraSphere The latter is an FDA approved treatment for primary liver cancer (HCC) which has been shown in clinical trials to increase survival rate of low-risk patients. SIR-Spheres are FDA approved for the treatment of metastatic colorectal cancer but outside the US SIR-Spheres are approved for the treatment of any non-resectable liver cancer including primary liver cancer.
- Intra-arterial iodine-131â€"lipiodol administration Efficacy demonstrated in unresectable patients, those with portal vein thrombus. This treatment is also used as adjuvant therapy in resected patients (Lau at et, 1999). It is believed to raise the 3-year survival rate from 46 to 86%. This adjuvant therapy is in phase III clinical trials in Singapore and is available as a standard medical treatment to qualified patients in Hong Kong.
- Percutaneous ethanol injection (PEI) well tolerated, high RR in small (<3Â cm) solitary tumors; as of 2005, no randomized trial comparing resection to percutaneous treatments; recurrence rates similar to those for postresection. However a comparative study found that local therapy can achieve a 5-year survival rate of around 60% for patients with small HCC.
- Combined PEI and TACE can be used for tumors larger than 4Â cm in diameter, although some Italian groups have had success with larger tumours using TACE alone.
- Portal Vein Embolization (PVE): Using a percutaneous transhepatic approach, an interventional radiologist embolizes the portal vein supplying the side of the liver with the tumor. Compensatory hypertrophy of the surviving lobe can qualify the patient for resection. This procedure can also serve as a bridge to transplant.
Complications: The most common complication of both TACE and SIRT is post embolization syndrome occurring in 60-80% of patients in TACE and 20-55% in SIRT. Typical findings of post embolization syndrome are fatigue, constitutional symptoms and abdominal pain. It usually lasts 3â€"4 days with full resolution in 7â€"10 days. Other more serious complications from TACE and SIRT include liver failure, hepatic dysfunction and gastric ulceration from non-target embolization of the left gastric. Less than 1% of patients who undergo SIRT develop radiation pneumonitis. Complications of RFA are rare but include abscess formation, subcapsular hematoma and tract seeding.
While surgical resection offers the best chance at a cure for hepatocellular carcinoma, the tumors are often inoperable due to large size or spread into vascular and adjacent structures. Medical management is generally palliative and aimed at reducing liver disease symptoms. Chemotherapy is traditionally ineffective. Interventional radiology offers minimally invasive treatments that can improve quality of life, increase survival, and reduce symptoms in these patients.
Other Management
- High intensity focused ultrasound (HIFU) (not to be confused with normal diagnostic ultrasound) is a new technique which uses much more powerful ultrasound to treat the tumour. Still at a very experimental stage. Most of the work has been done in China. Some early work is being done in Oxford and London in the UK.
- Hormonal therapy Antiestrogen therapy with tamoxifen studied in several trials, mixed results across studies, but generally considered ineffective Octreotide (somatostatin analogue) showed 13-month MS v 4-month MS in untreated patients in a small randomized study; results not reproduced.
- Adjuvant chemotherapy: No randomized trials showing benefit of neoadjuvant or adjuvant systemic therapy in HCC; single trial showed decrease in new tumors in patients receiving oral synthetic retinoid for 12 months after resection/ablation; results not reproduced. Clinical trials have varying results.
- Palliative: Regimens that included doxorubicin, cisplatin, fluorouracil, interferon, epirubicin, or taxol, as single agents or in combination, have not shown any survival benefit (RR, 0%-25%); a few isolated major responses allowed patients to undergo partial hepatectomy; no published results from any randomized trial of systemic chemotherapy.
- Cryosurgery: Cryosurgery is a new technique that can destroy tumors in a variety of sites (brain, breast, kidney, prostate, liver). Cryosurgery is the destruction of abnormal tissue using sub-zero temperatures. The tumor is not removed and the destroyed cancer is left to be reabsorbed by the body. Initial results in properly selected patients with unresectable liver tumors are equivalent to those of resection. Cryosurgery involves the placement of a stainless steel probe into the center of the tumor. Liquid nitrogen is circulated through the end of this device. The tumor and a half inch margin of normal liver are frozen to -190 °C for 15 minutes, which is lethal to all tissues. The area is thawed for 10 minutes and then re-frozen to -190 °C for another 15 minutes. After the tumor has thawed, the probe is removed, bleeding is controlled, and the procedure is complete. The patient will spend the first post-operative night in the intensive care unit and typically is discharged in 3 â€" 5 days. Proper selection of patients and attention to detail in performing the cryosurgical procedure are mandatory in order to achieve good results and outcomes. Frequently, cryosurgery is used in conjunction with liver resection as some of the tumors are removed while others are treated with cryosurgery. Patients may also have insertion of a hepatic intra-arterial catheter for post-operative chemotherapy. As with liver resection, the surgeon should have experience with cryosurgical techniques in order to provide the best treatment possible.
- Interventional radiology
- A systematic review assessed 12 articles involving a total of 318 patients with hepatocellular carcinoma treated with Yttrium-90 radioembolization. Excluding a study of only one patient, post-treatment CT evaluation of the tumor showed a response ranging from 29 to 100% of patients evaluated, with all but two studies showing a response of 71% or greater.
Prognosis
The usual outcome is poor, because only 10â€"20% of hepatocellular carcinomas can be removed completely using surgery. If the cancer cannot be completely removed, the disease is usually deadly within 3 to 6 months. This is partially due to late presentation with large tumours, but also the lack of medical expertise and facilities in the regions with high HCC prevalence. However, survival can vary, and occasionally people will survive much longer than 6 months. The prognosis for metastatic or unresectable hepatocellular carcinoma has recently improved due to the approval of sorafenib (Nexavar®) for advanced hepatocellular carcinoma.
Epidemiology
HCC is one of the most common tumors worldwide. The epidemiology of HCC exhibits two main patterns, one in North America and Western Europe and another in non-Western countries, such as those in sub-Saharan Africa, central and Southeast Asia, and the Amazon basin. Males are affected more than females usually and it is most common between the age of 30 to 50, Hepatocellular carcinoma causes 662,000 deaths worldwide per year about half of them in China.
Africa and Asia
In some parts of the world, such as sub-Saharan Africa and Southeast Asia, HCC is the most common cancer, generally affecting men more than women, and with an age of onset between late teens and 30s. This variability is in part due to the different patterns of hepatitis B and hepatitis C transmission in different populations - infection at or around birth predispose to earlier cancers than if people are infected later. The time between hepatitis B infection and development into HCC can be years, even decades, but from diagnosis of HCC to death the average survival period is only 5.9 months according to one Chinese study during the 1970-80s, or 3 months (median survival time) in Sub-Saharan Africa according to Manson's textbook of tropical diseases. HCC is one of the deadliest cancers in China where chronic hepatitis B is found in 90% of cases. In Japan, chronic hepatitis C is associated with 90% of HCC cases. Food infected with Aspergillus flavus (especially peanuts and corns stored during prolonged wet seasons) which produces aflatoxin poses another risk factor for HCC.
North America and Western Europe
Most malignant tumors of the liver discovered in Western patients are metastases (spread) from tumors elsewhere. In the West, HCC is generally seen as a rare cancer, normally of those with pre-existing liver disease. It is often detected by ultrasound screening, and so can be discovered by health-care facilities much earlier than in developing regions such as Sub-Saharan Africa.
Acute and chronic hepatic porphyrias (acute intermittent porphyria, porphyria cutanea tarda, hereditary coproporphyria, variegate porphyria) and tyrosinemia type I are risk factors for hepatocellular carcinoma. The diagnosis of an acute hepatic porphyria (AIP, HCP, VP) should be sought in patients with hepatocellular carcinoma without typical risk factors of hepatitis B or C, alcoholic liver cirrhosis or hemochromatosis. Both active and latent genetic carriers of acute hepatic porphyrias are at risk for this cancer, although latent genetic carriers have developed the cancer at a later age than those with classic symptoms. Patients with acute hepatic porphyrias should be monitored for hepatocellular carcinoma.
Research
Pre-clinical
Current research includes the search for the genes that are disregulated in HCC, protein markers, non-coding RNAs (such as TUC338) and other predictive biomarkers. As similar research is yielding results in various other malignant diseases, it is hoped that identifying the aberrant genes and the resultant proteins could lead to the identification of pharmacological interventions for HCC.
Clinical
JX-594, an oncolytic virus, has orphan drug designation for this condition and is undergoing clinical trials.
Abbreviations
HCC, hepatocellular carcinoma; TACE, transarterial embolization/chemoembolization; PFS, progression-free survival; PS, performance status; HBV, hepatitis B virus; PEI, percutaneous ethanol injection; RFA, radiofrequency ablation; RR, response rate; MS, median survival.





It is very good information about Radiological and Pathological services. Thank you sharing information.
ReplyDeleteRadiological and Pathological services
Happiness is all i see now I never thought that I will live on
ReplyDeleteearth before the year runs out. I have been suffering from a
deadly disease (Herpes) for the past 3 years now; I had spent
a lot of money going from one places to another, from
churches to churches, hospitals have been my home every day
residence. Constant checks up have been my hobby not until
this faithful day, I was searching through the internet, I saw a
testimony on how pp him +2348154637647 Dr Lucky, helped
someone in curing his Herpes disease, quickly I copied his
email which is (drluckyherbalcure@gmail.com) just to give
him a test I spoke to him, he asked me to do some certain
things which I did, he told me that he is going to provide the
herbal cure to me, which he did, then he asked me to go for
medical checkup after some days after using the herbal cure, I
was free from the deadly disease, he only asked me to post
the testimony through the whole world, faithfully am doing it
now, please brothers and sisters, he is great, I owe him in
return. if you are having a similar problem just email him on
(drluckyherbalcure@gmail.com) or Call him or WhatsApp him
+2348154637647
Can't still believe that i got cured from Genital Herpes through herbal treatment from Dr LUCKY who I met through the internet, I actually couldn't believe it at first because it sounded impossible to me knowing how far I have gone just to get rid of it. Dr LUCKY send me his medicine which I took as instructed and here I am living a happy life once again, a big thanks to Dr LUCKY , I am sure there are many herbal doctors out there but Dr LUCKY did it for me, contact him on Email him; { drluckyherbalcure@gmail.com }
ReplyDeletePowerful Herbal treatment is 100% guaranteed to cure Herpes Virus, The main reason why most people are finding it difficult to get cured from HSV 1& 2 is because they believe on medical treatment, i want you to know that drugs and medical treatments is not helpful to cure HSV permanently but it can only help you control it but the truth is in life time it will still be inside your nervous system, But Natural roots/herbs are the best remedy which can easily eradicate herpes forever. I never believed it until I was helped and cured of my 2 months genital herpes with natural herbal medicines from Dr. OKITI . Where other medical prescribed drugs and treatments failed, Dr. OKITI herbal medication helped me and cured me from herpes virus permanently and I’m so grateful for this. You can also get help from this great and powerful African Herbalist called Dr. OKITI by reaching him via email: Drokitiherbalhome100@gmail.com or call/whatsapp him at +234 705 067 0365. Thank you so much Dr. OKITI.
ReplyDeleteherpes is a serious and recurring disease which can't be cured through drugs or injections by the American doctors but the best way to deal with herpes is by taking natural herbs medicine for it and is only few American doctors that know about this herbal medicine from Dr Akhanene .. I have read about Dr Akhanene the great herbalist doctor from African who can cure disease with his powerful herbal medicine. for the people suffering from the following diseases, Herpes, Cancer, Also,Herpatitis, Diabetes, Hps,Infections ETC should contact him for his herbal medicine because i am a living testimony and i was cured of herpes. Although, i sent him what he requested and he sent me his medicine which i took for 1 weeks and today when i went for test i was tested herpes negative. you can reach him through his Emai drakhanenespellhome@gmail.com.com or whatsapp or call him +2348168714427
ReplyDeleteI never thought i would be HIV negative again after been diagnosed in 2017, i have tried everything possible in life from one doctor to another, one hospital to another, series of tests, different kinds of medication, i had already lost hope until i meet Great Dr. OSAGIE online testimonies, a specialist in herbal medication from Africa, i contacted him (drosagiesolutiontemple@gmail.com OR DROSAGIESOULTIONTEMPLE@YAHOO.COM) and he prepared HIV herbal medication for me which i took for 14days and now i am completely cured. i want to use this medium to express my gratitude to him for saving my life and curing me from HIV, for taking away all my pains and sorrows, I''m indeed grateful and i am so happy I''m now HIV negative. i will continue to tell the good news of your great works to everyone, if you have HIV or other disease contact him, Email: his email: (drosagiesolutiontemple@gmail.com OR DROSAGIESOULTIONTEMPLE@YAHOO.COM ) or Whatsapp number: +2347030465649 DOCTOR OSAGIE CAN AS WELL HELP THE FOLLOWING PROBLEMS
ReplyDelete1. HIV/AIDS SPELL
2. HERPES CURE OF KIND
3. CANCER SPELL
4 IF YOU WANT YOUR EX LOVER BACK SPELL
5 IF YOU NEED A BABY SPELL him to solve
6 LOW SPERM COUNT SPELL get all your problem solve. No problem is too big for him to solve.
ReplyDeleteA friend of mine recommended me to contact this herbal Doctor for herpes cure and he asked me to purchase his herbal medicine which i did, when i received this herbal medicine, he gave me instructions on how to use it, after taking the medicine as instructed for 2 weeks, i went for check up and the result shows negative and i was cured of herpes, I am now free from Herpes. You can contact him on his email …………His result is 💯💯💯💯💯 guaranteed. I highly recommend..........
You can win your Ex lover back in 48 hours just like me.
Very effective ...
For fast and reliable solution.
Get boyfriend back after break up.
Get girlfriend back after break up.
Get Gay partner back.
Get Lesbian partner back.
Make Your Husband/Wife love you Forever.
Stop Having Bad Dreams.
Make Women/Men To Run After You.
Stop Divorce from happening.
Divorce Your Husband/Wife.
Make Partner marry you.
Make Wishes To Be Granted.
Win Court Case/Law suit.
Get pregnant.
Luck To Win A Lottery.
Stop Marriage/Relationship from Breaking Apart.
I used his herbal remedy to cure Hsv-2..
100% result guaranteed..
Email R.buckler11 (( @gmail .com))…………